Stress, Mental Health, Harassment, & Bullying Hazard Awareness Resources (2026 Update)
*Please note this was originally written by the talented Beth Snyder in 2020. Jess Westra updated the phone numbers and links in 2026, added IATSE’s webinar channel, added some TTF resources, and removed a couple of COVID related links that are no longer active.
We all experience stress, it seems like a good time to change our mindset and try to do better by ourselves.
One way to do that is to check out the incredible variety of resources available through the IA and other organizations specifically designed to help displaced workers get through any mental issues they may currently be experiencing and also ways to deal with problems that may occur when working. The workshop provided a gigantic list of links to resources, which I will try to post a short explanation for each one (most will be quotes from their websites) so you have an idea if each one will help you or not.

Behind the Scenes Mental Health and Suicide Prevention Initiative: “Many people have become increasingly concerned about the rising number of suicides and the prevalence of alcohol/substance misuse within the entertainment industry. By its very nature our industry can impact your physical and emotional health due to long hours, pressure to push your body, and high workplace stress. In response, Behind the Scenes and other individuals and organizations have come together to create this initiative.”
HelpPro: Has created a searchable list of mental health professionals who either work (or have worked) in the entertainment industry themselves, or who have experience in counseling those who work in the industry.
iRel8 and Behind the Scenes: Partnership that produced “a mobile application that gives users an open and anonymous platform to receive mental health help, provide relevant advice to others, and relate to a larger community – all in a safe and non-identifiable way so a user’s reputation is not compromised in any way with friends, family members, or work colleagues.”
IATSE Education for All Webinar Channel: IATSE has recorded webinars on many helpful courses to help with your physical and mental needs, interpersonal relationships, and financial wellness. Much of our work is concentrated bursts of activity mixed with long periods of waiting. Mindful Muscle Memory help relieve the strain and strengthen your body. Also check out the Anxiety Toolbox, Beginner’s Guide to Therapy, and the Mental Health Toolbox. For those wanting to change the culture that is stressing them out, check out Straight Talk about Gay Pride, Unconscious Bias and Microaggressions, 60 to Zero in 60 Seconds: De-escalating Difficult Situations, and Equity, Diversity, and Inclusion Basics.
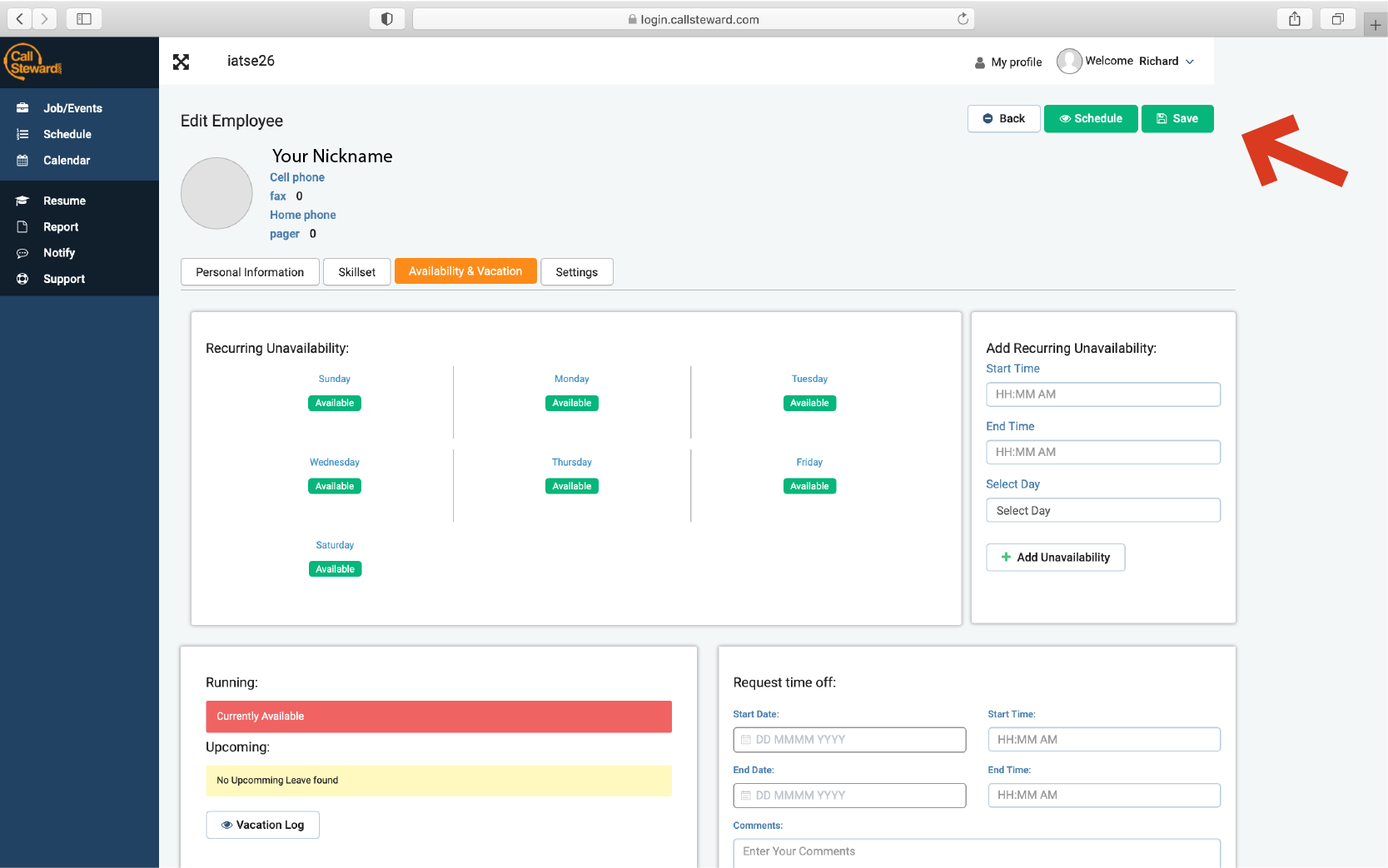
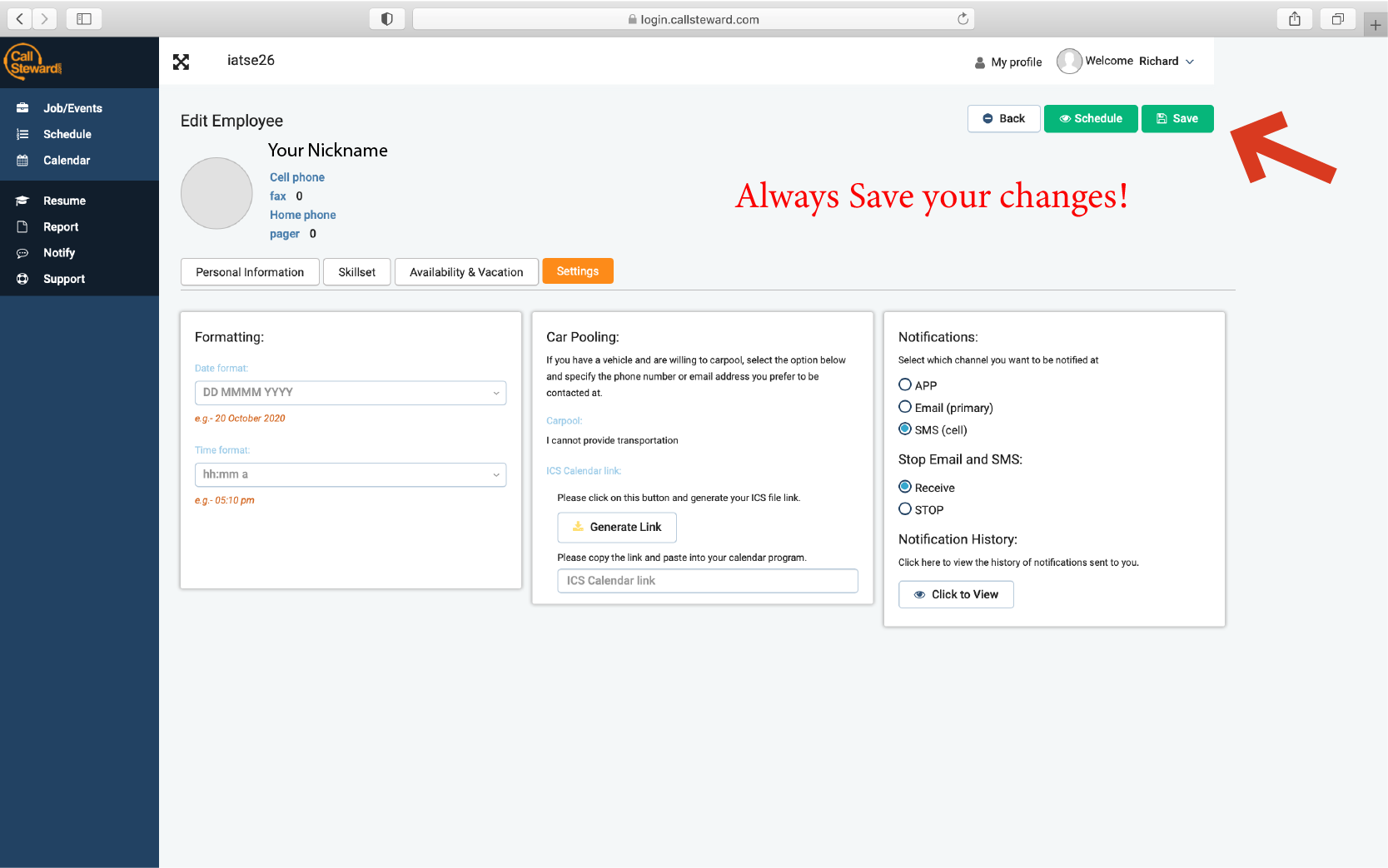
IATSE Local 26 is committed to protecting it’s workers. Please review the Workplace Behavior post. The Executive Board can only help with a situation or correct behavior if they know the problem exists.
For those that have applied for a (free to everyone on our referral list) IATSE Training Trust Courses and Resources account, you have access to craft skills courses on Customer Service for the Live Events Industry, Professional Etiquette, and STEP UP: Respect in the Workplace.
For those that have applied for a (free to everyone on our referral list) IATSE Training Trust’s LinkedIn Learning account, IATSE has several courses and learning paths available on teamwork, building an inclusive culture, managing your emotional response to workplace stress, and more. If you search for IATSE 26, there will be a learning path for conflict resolution. Try searching IATSE women, IATSE DEI, and/or IATSE Financial Wellness to see more options to empower yourself and those around you.
The Entertainment Community Fund: “Founded in 1882, The Actors Fund is a national human services organization here to meet the needs of our entertainment community with a unique understanding of the challenges involved in a life in the arts. Services include emergency financial assistance, affordable housing, health care and insurance counseling, senior care, secondary career development and more.”
Behind the Scenes Foundation: “Behind the Scenes was founded to provide assistance to entertainment technology professionals in need, no matter what color their skin, the language they speak, the religion they follow, or gender or sexuality they identify as. Our motto is, “Don’t leave your colleagues in the dark.” We want to shine a light into the dark corners of violence, hatred and injustice. We want to shine a light on this moment and the opportunity it represents; to become a better world that respects and protects the rights of every individual. A world that provides equal access to justice, economic opportunity, health care, and all-embracing social freedom.”
MusiCares: “MusiCares provides a safety net of critical assistance for music people in times of need. MusiCares’ services and resources cover a wide range of financial, medical and personal emergencies, and each case is treated with integrity and confidentiality. MusiCares also focuses the resources and attention of the music industry on human service issues that directly influence the health and welfare of the music community.”
Music Health Alliance: “Music Health Alliance serves all persons in the entertainment business nationwide in all genres of music who need assistance with medical bills or health guidance that includes finding doctors or prescription medicine, finding financial grants while recovering from a serious health issue, affordable health insurance, or answers to Medicare questions.”

American Psychological Association: Offers an extensive list of “COVID-19 resources for psychologists, health-care workers and the public.”
American Psychiatric Association : Provides resources for Patients and Families to “Learn about common mental disorders, including symptoms, risk factors and treatment options. Find answers to your questions written by leading psychiatrists, stories from people living with mental illness and links to additional resources.”
MentalHelp.net: “We’ve here collected resources concerned with helping people to manage disabilities. Given our psychological bent, where we’ve generated resources ourselves, they will focus on mental health in disability, although we’ve been much broader in selecting outside resources. We hope you’ll find this resource useful.”
Therapy for Black Girls: “The Therapy for Black Girls Podcast is a weekly chat about all things mental health, personal development, and all the small decisions we can make to become the best possible versions of ourselves.”
LGBTQ Psychotherapists of Color (QTOC): “QTOC is a San Francisco/Bay Area grassroots, volunteer-led group providing support, networking, leadership development, and community building opportunities for LGBTQs of Color in Psychology, Social Work, and Counseling.” While they are in the SF/Bay Area, they do offer virtual services.
Mental Health America: Mental Health America is the nation’s leading national nonprofit dedicated to the promotion of mental health, well-being, and condition prevention. MHA has compiled a range of resources and information. They have resources for different segments of the population to concentrate on their specific individual needs.
Drugwatch has published a guide on anxiety that covers: causes, common types, symptoms and tips for management/prevention titled “How to Deal with Anxiety”. It covers many reasons a person could feel anxiety, of course due to COVID-19, but also in general.
In Determining If You Need Drug Rehab Rehab Spot takes a look at the difference between tolerance, dependence, and addiction to drugs both legal and illegal, and offers several ways to get in touch with a rehab counselor should you feel you need one.
Social Work License Map has pulled together a collection of 60 digital resources for mental health help that “spans diagnostic tools, research portals, government organizations, nonprofits, blogs, and phone hotlines devoted to addressing issues ranging from general mental illnesses and disorders such as autism, anxiety, depression, eating disorders, and substance abuse, to the specific needs of diverse populations, including LGBTQ youth, minorities, women, and veterans.”
The Addiction Center recently published an article explaining how depression affects addiction, and also explains the difference between the different types of depression. Additionally, their website features many other sections about mental health and addiction.
Nurse Practitioners Online Improving Prevention and Survivor Outcomes: Resources for Human Trafficking Victims, Healthcare Workers and Colleges

There are also several phone numbers (and some you can text) for help dealing with whatever is bothering you. Sometimes it’s easier to reach out to someone anonymously over the phone or by text than to talk to someone you know or with whom you are face to face. However you feel comfortable talking to someone, please do so.
- Suicide and Crisis Lifeline: 988
- National Domestic Abuse Hotline: 1- 800-799-7233 or text BEGIN to 88788
- Crisis Text Line: Text REASON to 741741
- National Council on Alcoholism & Drug Dependency: 1-800-622-2255
- LGBT Hotline: 1-888-843-4564
- The Trevor Project: 1-866-488-7386 or text “START” to 678678 (Provides crisis intervention and suicide prevention services to lesbian, gay, bisexual, transgender, queer & questioning—LGBTQ—young people under 25.)
- Mental Health America Hotline: Text MHA to 741741
- The Childhelp National Child Abuse Hotline: (888) 721-3166
- Rape, Sexual Assault, Abuse, and Incest National Network (RAINN): (800) 656-HOPE or text HOPE to 64673
- Crisis Text Line From US & Canada: text HOME to 741741 to connect with a Crisis Counselor
We are all in this together, but we are all at different places mentally, financially, and physically. Please don’t feel you are alone, and please don’t feel you just need to “tough it out”. I’ve said it before and I’ll say it again… THERE IS NO SHAME IN NEEDING HELP. Reach out. There is help available, a lot of it for free. Don’t try to go it alone; there’s no need. Self-care is not a luxury, it is a necessity. Even if you don’t currently experience issues with depression, anxiety, or thoughts of self-harm, talking to someone can make you feel less disconnected from the world while we are out of work. A friend has called me a couple of times just to chat and see how I’m doing, and it’s made a huge difference in how I feel. And a lot of these resources will be helpful when we do get back to work, whenever that may be.
Now, what do we say?
Be safe. Be well. And as always… WASH YOUR HANDS!